Echolalia, sometimes called “echophrasia,” is the unsolicited repetition of words, phrases, or sentences heard from others — either immediately or after a delay. It is automatic, non-voluntary, and a normal part of early language development in toddlers (NIH StatPearls, 2023).
In most children, this repetitive speech pattern naturally decreases by around age 3. When it continues beyond this stage — particularly in children with autism spectrum disorder (ASD) — it may suggest the need for a speech therapy evaluation (Cleveland Clinic, 2025).
Repetitive language in children is common during speech and language development and is not always a cause for concern. Many children repeat words and phrases because they are still learning how language is processed and used. This guide explains the different types of echolalia, its possible causes, and how speech therapy can help children develop more meaningful and independent communication skills.
What Is Echolalia?
Echolalia refers to the repetition of words or phrases heard from another person, television show, song, or previous conversation. The term comes from the Greek words “echo” (repeat) and “lalia” (speech). In many children, this repeated speech happens automatically rather than intentionally.
Echolalia differs from palilalia in one important way. In palilalia, a person repeatedly says their own words or sounds, whereas in echolalia the repeated language comes from an outside source or another speaker.
Imitation plays an important role in language development. Toddlers usually begin by copying sounds, then words, and eventually form their own sentences. Research referenced by NIH and ASHA shows that up to 75% of verbal children with autism display this type of repetition at some stage of development. Current estimates suggest prevalence can range from 25% to 91%, depending on the diagnostic criteria used (Sutherland et al., Current Developmental Disorders Reports, 2024).
This behaviour is not limited to autism. Many typically developing toddlers also repeat words and phrases while learning to communicate.
Echolalia is a recognised stage of language development and does not always mean autism.

Types of Echolalia
Immediate Echolalia
Immediate echolalia occurs when a child repeats something right after hearing it. You ask, “Do you want juice?” and the child says, “Do you want juice?” back. In many cases, this type of repetition helps the child process language, participate in conversation, or understand what was said. However, therapists may become concerned when the child cannot produce original responses independently.
Delayed Echolalia
Delayed echolalia refers to repeating words or phrases heard hours, days, or even weeks earlier. For example, a child may repeat a line from a cartoon during dinner even when the programme is not playing.
Unlike immediate repetition, these phrases are stored in memory and used later in different situations. Delayed scripting often carries meaning, with the child using familiar language patterns to express emotions, needs, or experiences.
Some children also display ambient repetition, where they repeat conversations or words overheard in the environment without anyone speaking directly to them.
Mitigated Echolalia
Mitigated echolalia occurs when a child begins modifying parts of a repeated phrase. For instance, after hearing “Do you want a biscuit?” the child may respond with “Want biscuit.”
According to NIH StatPearls (Patra & De Jesus, 2023), this is considered a positive developmental sign because the child is beginning to process and adapt language rather than repeating it word-for-word.
As a result, this stage suggests progress from fixed scripted speech toward more flexible and independent language use.
Communicative and Semi-Communicative Forms
Speech-language therapists commonly classify repetitive language into communicative and semi-communicative forms. Communicative repetition serves a clear purpose, such as requesting help, asking for something, or participating socially.
Semi-communicative repetition may not seem meaningful initially, but it often helps the child regulate emotions, process sensory information, or internally rehearse language. Both forms provide important insight into how the child understands and organises communication.
What Causes Echolalia in Children?
At its core, echolalia reflects the way some children process, store, and organise language before they are able to generate spontaneous speech independently. Several developmental and neurological conditions may be associated with this pattern of communication:
- Autism Spectrum Disorder (ASD): The most common association. Many children with ASD rely on gestalt language processing and may struggle with generating spontaneous speech naturally.
- Global developmental language delay: Some children use repeated phrases as a bridge while their original language and communication skills continue developing.
- Cerebral palsy: Motor speech and communication difficulties can sometimes lead to repetitive speech patterns. Read more about cerebral palsy types and early treatment.
- Anxiety and sensory overload: Repetitive language often increases during stress or overstimulation. Familiar phrases may help the child feel regulated and secure.
- Tourette syndrome: Both echolalia and echopraxia (repetition of movements or actions) are recognised characteristics of Tourette syndrome (TS).
Do not assume a diagnosis based on echolalia alone. A professional speech and developmental evaluation is necessary to understand the underlying reason for the behaviour.
Echolalia is a symptom, not a diagnosis — the root cause can only be identified through a proper clinical assessment.
Is Echolalia a Problem or a Communication Attempt?
Research shows that echolalia is often meaningful communication rather than random repetition.
For example, a child may say “Wheels on the bus” to ask to go outside because they associate the song with car rides. Similarly, another child may repeat “Do you want to play some more?” to mean they want to stop an activity. Meanwhile, some children repeat “It’s time for dinner” at mealtime as part of a familiar routine.
Stages of Language Development in Echolalia
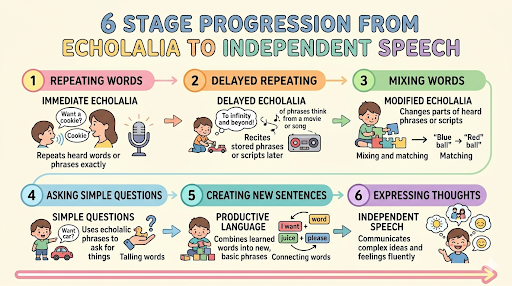
NIH StatPearls (2023) outlines the natural progression from echolalia to independent language:
Stage 1: Whole gestalt phrases — child repeats complete sentences heard in context (e.g., “Do you want more juice?”)
Stage 2: Mitigated echolalia — child begins altering the phrase (e.g., “Want more juice”)
Stage 3: Isolation of single words; two-word combinations (e.g., “Want juice”, “More please”)
Stage 4: First simple original sentence (e.g., “I want juice”)
Stage 5: Complex sentences with grammar (e.g., “Can I have some juice please?”)
Stage 6: Advanced grammar and fully flexible language
Importantly, Speech therapy accelerates progress through these stages. Rather than skipping echolalia, therapists focus on guiding the child forward along this documented developmental path.
Echolalia becomes a genuine barrier only when it replaces all communication — when the child has no other way to express any need. Even then, the answer is not silence. The answer is building new options.
Many children naturally move from echolalia toward independent speech with the right support.
Can Speech Therapy Reduce Echolalia?
Yes — but with an important distinction. The goal of speech therapy for echolalia is not to eliminate repetition overnight. The goal is to build spontaneous, functional language so the child relies on scripted phrases less and less. Removing echolalia without offering a communication replacement leaves the child with nothing.
According to NIH StatPearls (2023), echolalia should be viewed as a positive sign for language development in children with ASD, and early evidence-based intervention is necessary to enhance outcomes.
Also Read: Benefits of Occupational Therapy for Autism in Kids
Research consistently shows that early, targeted intervention reduces reliance on echolalic speech and promotes natural language use (GoldStar Rehab, 2024).
Children who begin speech therapy for echolalia before age 5 show significantly greater gains in spontaneous language than those who start later (NIH, 2023).
Why Early Speech Therapy Matters for Echolalia
Modelling and Expansion
Rather than correcting the echo, the therapist builds on it. If a child says “Want juice want juice,” the therapist models “I want juice please.” This validates what the child said and offers a slightly expanded version for them to absorb over time.
Functional Communication Training (FCT)
FCT identifies what the child is trying to say through echolalia, then teaches a clearer way to express it. This directly reduces the functional need for scripted repetition.
Cues-Pause-Point Training
The therapist gives a cue, pauses for several seconds, then points to prompt an original response. A systematic review by ASHA found that this technique consistently reduced echolalia across all studies reviewed, while tact-training both reduced echolalia and increased spontaneous speech (ASHA Evidence Maps, 2025). The pause matters — it removes the pressure that triggers scripted echoing.
Script Fading and Visual Supports
Script fading uses the child’s existing scripted phrases as a starting point, then gradually introduces variation until new language combinations emerge. Visual supports — picture cards, PECS, communication boards — give the child an alternative channel to express needs, reducing pressure on verbal output.
Parent-Mediated Therapy
Parents are trained to respond to echolalia in ways that encourage expansion. What happens between sessions is just as important as the session itself. PediGym’s early intervention programme includes parent coaching as a core component of every speech therapy plan. For practical home exercises you can try right away, see our guide on speech therapy exercises at home.
How to Reduce Echolalia at Home
These strategies will not replace therapy, but they will meaningfully support it:
- Respond to the intent, not the words. Ask yourself what the child is trying to say, then respond to the meaning behind the echo.
- Offer choices, not open questions. “Juice or water?” is easier to respond to than “What do you want?” — it reduces anxiety and gives the child a language template.
- Pause and wait. After speaking, count to 10 before prompting again. During this window, original responses often begin to emerge.
- Keep sentences short. Simpler input is easier to process. Long sentences increase cognitive load and make echoing more likely.
5. Praise every spontaneous word. Any phrase that is not an echo deserves genuine, immediate praise. It builds the child’s confidence in their own voice.

Echolalia and Developmental Milestones
Developmental context matters. The same behaviour that is normal at 18 months is a clinical signal at 4 years. Here is what to expect at each stage:
- Ages 0–2: Echolalia is usually a normal part of early language development. Babies and toddlers learn communication by copying sounds, words, and short phrases they hear around them.
- Ages 2–3: Some repetitive speech is still expected, especially immediate repetition during play or conversation. However, children should also begin using original words and simple two-word phrases. If repeated scripting is the child’s only way of communicating, consider an evaluation with a speech-language pathologist.
- Age 3 and beyond: Persistent echolalia with limited or no spontaneous speech may require formal evaluation. At this stage, professionals most commonly identify communication difficulties linked with ASD, developmental delay, or related conditions. Early referral at this point leads to the best outcomes.
When Should You See a Speech Therapist for Echolalia?
You do not need a formal diagnosis before booking an assessment. A speech-language pathologist can evaluate echolalia and related communication concerns independently. Consider seeking professional advice if:
- Echolalia is still present and not reducing after age 3
- Your child has no spontaneous or original words at all
- Repetitive speech occurs along with limited eye contact, social withdrawal, or not responding to their name
- Your child previously used words but has lost them
- The repetition is increasing rather than improving
The American Academy of Pediatrics recommends developmental screening at 18 and 24 months. Cleveland Clinic (2025) also advises seeking professional guidance if repetitive speech continues after age 3 or reappears after earlier language improvement.
If your child also shows signs of difficulty with pronunciation or unclear speech alongside echolalia, our blog on misarticulation therapy and occupational therapy for children may be relevant to your situation.
Early assessment is the single most impactful step a parent can take when echolalia persists beyond age 3.
How PediGym Helps Children with Echolalia
At PediGym, every child starts with a structured assessment — not a generic plan. We identify the type of echolalia, its communicative function, and any co-occurring sensory or motor factors. Therapy typically combines speech therapy for kids with parent-mediated strategies and, where relevant, occupational therapy. All therapy is supervised by Dr. Nitin Gupta, DMI Level C Certified Therapist and Founder of PediGym. We have centres in Faridabad (Sector 85 and Sector 17) and Gurgaon (DLF Phase 2). A free initial consultation is available.
Frequently Asked Questions
Is echolalia always a sign of autism?
No. Echolalia can occur in typically developing toddlers as well as in children with Tourette syndrome, cerebral palsy, developmental delays, and other conditions. A professional evaluation is needed to identify the underlying cause.
At what age should echolalia stop?
Most children naturally move beyond echolalia by age 3. If it continues after this age — or returns after previously improving — consult a speech-language pathologist.
What is the difference between echolalia and palilalia?
Echolalia involves repeating words heard from another person or source. Palilalia involves repeating one’s own words or sounds. Both may occur in ASD and Tourette syndrome but have different neurological causes.
What is the difference between immediate and delayed echolalia?
Immediate echolalia happens right after hearing something. Delayed echolalia occurs hours, days, or weeks later, often using remembered phrases from TV shows, conversations, or advertisements.
Can speech therapy reduce or stop echolalia?
Yes. Speech therapy helps children develop spontaneous and functional communication so they rely less on repeated scripting. Techniques like modelling and Cues-Pause-Point training are especially effective (ASHA Evidence Maps, 2025; NIH StatPearls, 2023).
Where can I find a speech therapist for echolalia in Faridabad or Gurgaon?
PediGym has specialist centres in Faridabad (Sector 85 and Sector 17) and Gurgaon (DLF Phase 2). Contact us at pedigym.com/contact/ or call +91 98739 71012. Free initial consultation available.
Will echolalia go away on its own without therapy?
In many typically developing children, yes — repetitive speech usually fades by age 3 as language develops. In children with ASD or developmental delays, structured speech therapy is often needed to build independent communication skills.
Final Word
This behaviour is not limited to autism. Many typically developing toddlers also repeat words and phrases while learning to communicate. Overall, echolalia is a recognised stage of language development and does not always indicate autism.
Contact PediGym today for a free consultation at our centres in Faridabad and Gurgaon — pedigym.com/contact/.

Dr. Nitin, Founder of PediGym Child Development Center, is a dedicated pediatric therapy expert and DMI Level C Certified Therapist leading structured, evidence-based therapy programs in Faridabad and Gurgaon. Under his guidance, PediGym provides comprehensive pediatric rehabilitation focused on improving motor skills, coordination, sensory processing, speech clarity, and functional independence through personalized intervention plans.